1. WHAT IS THIS DATA RESOURCE CALLED AND HOW SHOULD IT BE CITED?
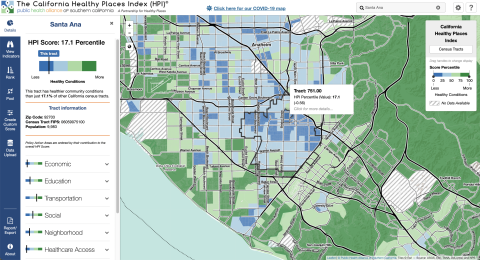
margauxfPublic Health Alliance of Southern California. California Healthy Places Index. 2019. https://healthyplacesindex.org.
© 2018 Public Health Alliance of Southern California
Permission is hereby granted to use, reproduce, and distribute these materials for noncommercial purposes, including educational, government and community uses, with proper attribution to the Public Health Alliance of Southern California including this copyright notice. Use of this publication does not imply endorsement by the Public Health Alliance of Southern California.
© 2018 California Department of Public Health (CDPH)
Permission is hereby granted to use, reproduce, and distribute these materials for noncommercial purposes, including educational, government, and community uses, with proper attribution to the CDPH, including this copyright notice. Use of this publication does not imply endorsement by the CDPH.