Empirical data
Taina Miranda AraujoIn response to
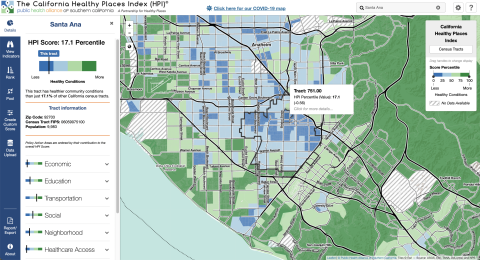
Studie provides visual representations of lead concentration in Santa Ana cross matching it with vulnerability risk.
Studie provides visual representations of lead concentration in Santa Ana cross matching it with vulnerability risk.
“Also of note when interpreting our results is that this study did not take into consideration the ingestion of heavy metals through the dietary route. Had we considered this additional exposure pathway, our calculated chronic daily intake levels of heavy metals would have been greater, resulting in higher estimated risk (particularly for metals such as Pb, As, and Cd which have been widely documented in various foods)” (Marsi et al. 2021)
“Both cancer and non-cancer risk at the Census tract level exhibited positive correlations with indicators of social as well as physiological vulnerability” (Marsi et al. 2021)
Exposure to heavy metals has been associated with adverse health effects and disproportionately impacts communities of a lower socio-economic status.
This study used a community-based participatory research approach to collect and analyze a large number of randomly sampled soil measurements to yield a high spatially resolved understanding of the distribution of heavy metals in the Santa Ana soil, in an effort to exposure misclassification. This study looks into average metal concentrations at the Census tract level and by land use type, which helps map potential sources of heavy metals in the soil and better understand the association between socioeconomic status and soil contamination (Marsi et al. 2021).
In 2018, soil samples of eight heavy metals including lead (Pb), arsenic (As), manganese (Mn), chromium (Cr), nickel (Ni), copper (Cu), cadmium (Cd), and zinc (Zn) were collected across Santa Ana. These were analyzed at a high resolution using XRF analysis. Then, metal concentrations were mapped out and American Community Survey data was used to assess the metals throughout Census tracts in terms of social and economic variables. Risk assessment was conducted to evaluate carcinogenic risk. The results of the concentrations of soil metals were categorized according to land-use type and socioeconomic factors. “Census tracts where the median household income was under $50 000 had 90%, 92.9%, 56.6%, and 54.3% higher Pb, Zn, Cd, and As concentrations compared to high-income counterparts” (Marsi et al. 2021). All Census tracts in Santa were above hazard inder >1, which implies non-carcinogenic effects, and almost all Census tracts showed a cancer risk above 104, which implies greater than acceptable risk. Risk was found to be driven by childhood exposure.
It was concluded that the issue of elevated soil contamination relates back to environmental justice due to overlap between contaminated areas and neighborhoods of lower socioeconomic status. Marsi et al. (2021) found there needs to be more community-driven recommendations for policies and other actions to address disproportionate solid contamination and prevent adverse health outcomes.
Published in May 2021, amid the coronavirus pandemic where in-person community workshops and meetings turned into weekly virtual meetings.
-> Authors:
Shahir Masri: Department of Environmental and Occupational Health, Program in Public Health, University of California, Irvine; air pollution scientist.
Alana M. W. LeBrón: Department of Health, Society, and Behavior, University of California, Irvine; Assistant Professor, Chicano/Latino Studies; Interests: structural racism and health, health of Latina/o communities, community-based participatory research.
Michael D. Logue: Department of Chicano/Latino Studies, University of California, Irvine
Enrique Valencia: Orange County Environmental Justice, Santa Ana
Abel Ruiz: Jóvenes Cultivando Cambios, Santa Ana; CRECE Urban Farming Cooperative member
Abigail Reyes: Community Resilience, University of California, Irvine
Jun Wu: Department of Environmental and Occupational Health, Program in Public Health, University of California, Irvine
Public Health Alliance of Southern California. California Healthy Places Index. 2019. https://healthyplacesindex.org.
© 2018 Public Health Alliance of Southern California
Permission is hereby granted to use, reproduce, and distribute these materials for noncommercial purposes, including educational, government and community uses, with proper attribution to the Public Health Alliance of Southern California including this copyright notice. Use of this publication does not imply endorsement by the Public Health Alliance of Southern California.
© 2018 California Department of Public Health (CDPH)
Permission is hereby granted to use, reproduce, and distribute these materials for noncommercial purposes, including educational, government, and community uses, with proper attribution to the CDPH, including this copyright notice. Use of this publication does not imply endorsement by the CDPH.
The index does not include certain neighborhood characteristics critical to health because they did not meet the criteria for inclusion (described in question 3). For instance, this included physician ratios (the number of physicians per 100,000 population) because data was missing for a majority of census tracts. In fact, the steering committee was unable to locate much data on health care access or quality at the census-tract level (only data on health care insurance coverage was available).
The index was previously critiqued in ways that led to a shift from framing data in terms of “disadvantage” towards a framework of “opportunity”. This led to not only a renaming of the index (from “the Health Disadvantage Index to the Healthy Places Index) but also a shift in reporting of data (e.g. highlight the percentage of the population with a BA degree or higher rather than the percentage of population without a college degree).
The HPI is also limited in terms of the effects of confounding, with some indicators with strong evidence of health effects showing contrary associations with life expectancy at birth by census tract. The steering committee has also acknowledged that the HPI might not be accurate for census tracts undergoing rapid population change (e.g. due to immigration, rapid gentrification, or other changes).
The HPI notably does not correlate strongly with CalEnviroScreen, which the steering committee for the HPI noted failed to identify one-third of census tracts with the worst conditions for population health. The HPI is ultimately more centered on considering environmental factors as a part of overall health, rather than as a central determinant. However, this disconnect between CalEnviroScreen and the HPI may also be a reflection of the challenges environmental injustice advocates have faced in linking environmental factors to health outcomes (which might not be as visible and geographically direct as the links between health and other indicators).
The HPI draws data about 25 community characteristics into a single indexed HPI score. The includes sub-scores for 8 “Policy Action Areas”: Economic, Education, Housing, Health Care Access, Neighborhood, Clean Environment, Transportation, and Social Factors. These scores are meant to be used to evaluate health geographically. Each policy action area includes the following individual indicators and weights:
ECONOMIC (0.32)
EDUCATION (0.19)
HEALTHCARE (0.05)
HOUSING (0.05)
NEIGHBORHOOD (0.08)
CLEAN ENVIRONMENT (0.05)
SOCIAL (0.10)
TRANSPORTATION (0.16)
*The steering committee for the HPI sought to include race/ethnicity as a 9th policy action area, but they were prohibited from doing so by state law which does not allow California state agencies to use race as a basis for public contracting.
The primary HPI Index is designed to align with life expectancy at birth as a predictive measure of community health status. However, the Healthy Places mapping tool can also be used to create custom scores using different indicators. The mapping tool includes detailed definitions of each indicator.
Each indicator is linked to a policy guide, which outlines concrete actions (e.g. best practices, emerging policy options) that local jurisdictions can take to improve HPI indicators. These actions are sometimes aimed at addressing direct links between policy and an action area, and other times aimed at addressed the root causes of an action area. The mapping tool also enables filtering results by “Decision support layers” like health outcomes, health risk behaviors, race/ethnicity, climate change effects, and other layers that the alliance identifies as important for advancing “resilient, equitable communities in California”. Geographies (e.g. census tracts) can also be compared by indicator using a ranking tool. The pool function can be used to create customized aggregations of data to map (e.g. adding several census-tracts together).
Data is available at several different scales: census-tracts, congressional districts, state assembly districts, state senate districts, cities, core based statistical areas, elementary school districts, metropolitan planning organization and medical service study areas.